
Sports-related groin injuries: a complete athlete's guide
- 3 hours ago
- 8 min read

TL;DR:
Sports-related groin injuries involve overload or damage to various groin structures and require accurate classification for effective treatment. Proper diagnosis relies on clinical assessment and imaging, with exercise programs like the Copenhagen Adduction Exercise playing a key role in prevention. Gradual, criterion-based rehabilitation ensures safe return to play and reduces the risk of recurrence.
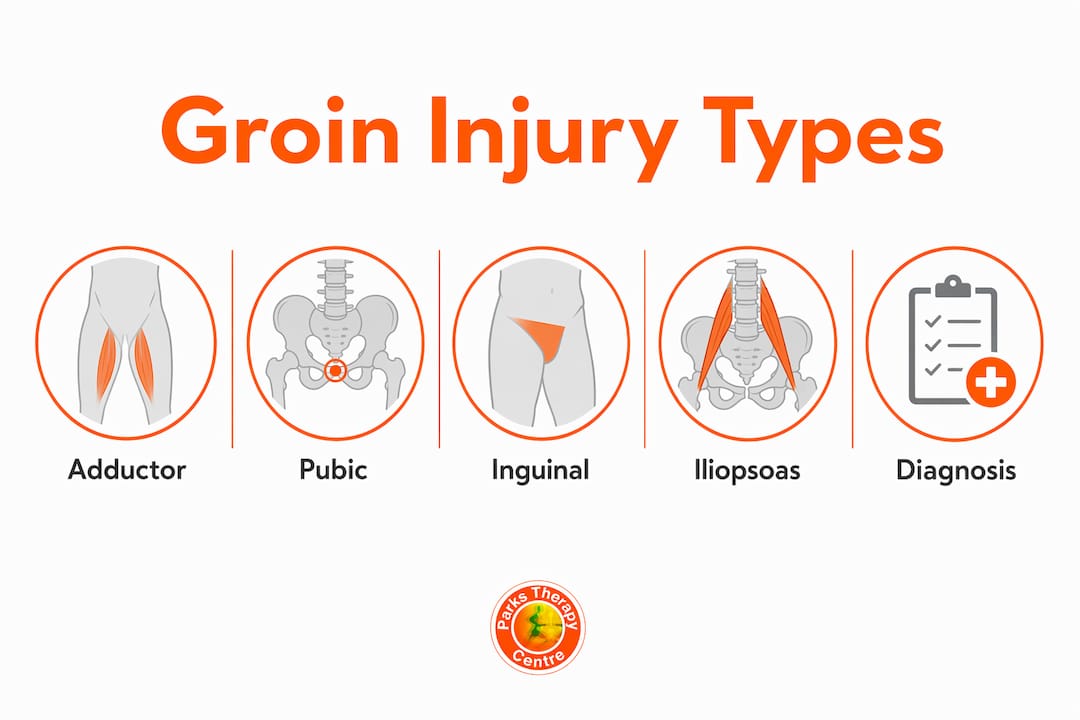
Sports-related groin injuries are defined as pain in the groin region arising from overload or damage to one or more anatomical structures including the adductors, pubic symphysis, inguinal canal, or iliopsoas muscle. The Doha Agreement framework classifies these into four primary clinical entities, each requiring a different management approach. Understanding sports-related groin injuries matters because misdiagnosis leads to prolonged absence from sport and a higher risk of recurrence. Athletes in high-intensity pivoting sports such as football, rugby, and ice hockey face the greatest exposure to these injuries.
What are the common types and symptoms of sports-related groin injuries?
Groin pain in athletes is clinically categorised into four primary entities, with MRI as the preferred imaging modality. Each type has a distinct anatomical basis and a characteristic symptom pattern.
Adductor-related groin pain
Adductor-related pain is the most common type in field sport athletes. It presents as medial groin pain reproduced by resisted hip adduction. The adductor longus tendon is the most frequently involved structure. Athletes typically report a sharp pull during sprinting, cutting, or kicking.

Pubic-related groin pain
Pubic-related pain originates at or around the pubic symphysis. Athletes describe a deep, central ache that worsens with trunk loading and single-leg activities. Athletic pubalgia results from pelvic and core stability overload, and MRI confirms characteristic musculotendinous injuries while excluding other causes. Diagnosis is often delayed because symptoms overlap with adductor and inguinal presentations.
Inguinal-related groin pain
Inguinal-related pain sits in the inguinal canal region and is aggravated by Valsalva manoeuvres, coughing, and explosive acceleration. A common misconception is that this equals a hernia. Inguinal-related groin pain often lacks a true hernia; it usually reflects muscle, tendon, or fascial overload rather than a structural defect. The term “sports hernia” is frequently a misnomer and can lead athletes toward unnecessary surgical consultations.
Iliopsoas-related groin pain
Iliopsoas-related pain presents as anterior hip and groin discomfort, reproduced by resisted hip flexion or passive hip extension stretching. It is less common than adductor-related pain but is frequently missed in athletes who present with anterior groin symptoms.
Key signs that distinguish the four types include:
Adductor-related: pain on resisted adduction, tenderness at the adductor longus origin
Pubic-related: pain on resisted trunk flexion, tenderness directly over the pubic symphysis
Inguinal-related: pain reproduced by Valsalva, no palpable hernia, inguinal canal tenderness
Iliopsoas-related: pain on resisted hip flexion, anterior hip tenderness, pain with passive extension
Dynamic ultrasound complements MRI for inguinal pain assessment, particularly when real-time movement provocation is needed to identify subtle structural changes.
How are sports-related groin injuries diagnosed and evaluated?
Accurate diagnosis of common groin injuries starts with a thorough clinical history and physical examination. Imaging supports clinical reasoning but does not replace it.
The clinical assessment should establish which movements provoke pain, how long symptoms have been present, and whether the athlete has had previous groin problems. Key physical tests include:
Resisted adduction test: reproduces adductor-related pain; performed supine with the examiner resisting hip adduction
Resisted trunk flexion: targets pubic-related pain by loading the rectus abdominis insertion at the pubic crest
Valsalva manoeuvre and inguinal canal palpation: identifies inguinal-related pain without a true hernia
Resisted hip flexion: screens for iliopsoas involvement, particularly in athletes with anterior groin symptoms
MRI remains the gold standard for confirming tissue involvement and excluding serious pathology such as stress fractures or avulsion injuries. Dynamic ultrasound adds value when inguinal canal integrity needs real-time assessment during provocative movements.
Early imaging may identify asymptomatic abnormalities, so clinical assessment must guide interpretation to avoid overdiagnosis. Many scan findings appear in athletes who have no symptoms at all. A positive MRI finding without a corresponding clinical picture does not confirm a diagnosis.
Pro Tip: If your scan shows a finding but your symptoms do not match the location or provocation pattern, ask your physiotherapist to reassess the clinical picture before accepting the imaging result as the definitive diagnosis.
Clinicians at Parkstherapycentre use a structured assessment process that links symptom location and provocative tests to likely tissue involvement, which guides targeted rehabilitation priorities rather than relying on imaging alone.
What exercise and prevention strategies reduce groin injury risk?
Exercise interventions are the primary method of groin injury prevention, though evidence for risk reduction is limited and no single exercise offers guaranteed protection. Dosing and progression are the critical variables that determine whether a prevention programme works.
The Copenhagen Adduction Exercise (CAE) is the most widely studied intervention for adductor-related groin pain. A 2026 systematic review found that CAE improved eccentric hip adduction strength, hip range of motion, dynamic balance, and reduced symptoms. Effectiveness was directly linked to training volume and progressive overload. A low-dose CAE programme performed sporadically provides little benefit.
Here is a practical framework for implementing groin injury prevention exercises:
Start with the Copenhagen Adduction Exercise in its easiest progression. Begin with the short-lever version (knee on bench) before advancing to the long-lever version (ankle on bench). This protects athletes who have low baseline adductor strength.
Progress the load every two to three weeks. Add repetitions before increasing lever length. Stagnating at the same progression for months is the most common error in team sport settings.
Combine CAE with hip flexor and core loading. Multifaceted exercise programmes combining CAE with other interventions may offer improved prevention outcomes compared to CAE alone. Include exercises such as side-lying hip adduction, single-leg deadlifts, and Copenhagen planks.
Integrate prevention work into warm-ups. CAE is field-friendly and suitable for warm-ups or strength programmes in team sports. Embedding it into the pre-training routine improves compliance.
Monitor for groin soreness after sessions. A soreness score above 3 out of 10 the morning after training is a signal to reduce load, not to stop the programme entirely.
Pro Tip: Athletes who stop their prevention programme as soon as symptoms disappear are the ones most likely to re-injure. Continue structured loading for at least six weeks after symptoms resolve to build the tissue capacity needed to withstand full training demands.
For a more detailed breakdown of evidence-based prevention strategies, Parkstherapycentre has published a practical guide covering exercise selection and progression for field sport athletes.
How should athletes approach rehabilitation and return to play?
Sports injury rehabilitation for groin injuries follows a phased timeline. Structured rehabilitation progresses from the acute phase (days 1–7) through functional conditioning (weeks 6–12) to return to play (week 12 and beyond). Pain reduction alone is not sufficient to clear an athlete for full training.
The phases break down as follows:
Acute phase (days 1–7): Reduce pain and swelling. Avoid provocative loading. Begin pain-free isometric adductor contractions to maintain neural drive.
Early loading phase (weeks 2–5): Introduce progressive isotonic adductor and hip flexor exercises. Begin low-impact cardiovascular work such as cycling or swimming.
Functional conditioning phase (weeks 6–12): Progress to sport-specific movements including lateral shuffles, change-of-direction drills, and controlled kicking or sprinting. Load should increase weekly if pain remains below 3 out of 10.
Return-to-play phase (week 12+): Reintroduce full training volume. Complete functional performance testing before clearance.
Return-to-play decisions should be criterion-based, heavily weighting pain assessments during resisted contractions and sport-specific on-field tests. Successful completion of a full high-demand team training session is recommended before final clearance. This is a non-negotiable gate because it replicates the physical and cognitive demands of competition.
Rehabilitation phase | Key criteria to progress |
Acute (days 1–7) | Pain-free at rest; no swelling increase |
Early loading (weeks 2–5) | Pain below 3/10 during isotonic exercises |
Functional conditioning (weeks 6–12) | Sport-specific drills pain-free; strength symmetry improving |
Return to play (week 12+) | Full team training completed; resisted strength tests passed |
The role of physiotherapy in groin recovery is to guide progression through each phase, adjust loading when setbacks occur, and confirm readiness using objective tests rather than subjective athlete confidence alone. Premature return is the single biggest driver of re-injury in groin conditions.
For athletes building their first structured plan after injury, Parkstherapycentre’s guide on post-injury training plans provides a practical framework for progressing safely back to full sport.
Key takeaways
Effective management of sports-related groin injuries requires accurate classification of the injury type, evidence-based exercise programming, and criterion-based return-to-play protocols rather than symptom-driven decisions.
Point | Details |
Four distinct injury types | Adductor, pubic, inguinal, and iliopsoas injuries each need targeted treatment. |
Imaging supports, not replaces, clinical assessment | Asymptomatic scan findings are common; always correlate with physical examination. |
CAE requires progressive overload | The Copenhagen Adduction Exercise only reduces risk when dosed and progressed correctly. |
Rehab phases are non-negotiable | Progressing too early after pain resolves is the leading cause of re-injury. |
Criterion-based return to play | Full high-demand team training must be completed before clearance for competition. |
What I have learned from working with groin injuries over the years
The most consistent error I see is treating groin pain as a single condition. An athlete who has adductor-related pain needs a completely different loading programme from one with inguinal-related symptoms. Conflating the two wastes weeks of rehabilitation time and often makes the less-treated condition worse.
The second pattern I see repeatedly is athletes stopping their strengthening programme the moment pain drops. Pain reduction is not tissue recovery. The adductor longus tendon, for example, needs weeks of progressive loading beyond the point of symptom resolution to rebuild the capacity required for sprinting and cutting. Stopping early is the most predictable route back to the treatment table.
What actually works is a structured, progressive programme that continues well past the point of comfort. It requires honest communication between the physiotherapist, the athlete, and the coaching team. Coaches need to understand why an athlete is not yet cleared for full training, and athletes need to trust that the criteria exist for good reason. When all three parties are aligned, return-to-play timelines shorten and recurrence rates drop.
The clinical differentiation insights from musculoskeletal specialists reinforce this point: groin and hip pain overlap significantly, and the athletes who recover fastest are those whose clinicians take the time to identify the specific structure involved rather than treating the region as a whole.
— Ivan
Parkstherapycentre: expert support for groin injury recovery
Groin injuries respond best to care that is specific to the tissue involved and the demands of your sport. Parkstherapycentre has been delivering physiotherapy and sports injury treatment since 1986, with clinics across Bedfordshire and Buckinghamshire.

The team at Parkstherapycentre provides structured groin injury assessments, progressive rehabilitation programmes, and return-to-play planning tailored to your sport and training schedule. Whether you are managing a new adductor strain or dealing with a recurring pubic-related problem, expert physiotherapy gives you a clear, evidence-based path back to full performance. Book an assessment at Parkstherapycentre and get a rehabilitation plan built around your specific injury, not a generic protocol.
FAQ
What are the four types of sports-related groin pain?
The four types are adductor-related, pubic-related, inguinal-related, and iliopsoas-related groin pain, as defined by the Doha Agreement framework. Each type involves different anatomical structures and requires a targeted rehabilitation approach.
What are the signs of a groin strain in athletes?
The main signs of a groin strain include medial groin pain during or after sprinting and kicking, tenderness at the adductor longus origin, and pain reproduced by resisted hip adduction. Swelling and bruising may appear in more severe cases.
Is a sports hernia the same as a groin strain?
A sports hernia is not the same as a groin strain. The term is frequently a misnomer; inguinal-related groin pain usually reflects muscle, tendon, or fascial overload rather than a true hernia, and most cases respond to conservative physiotherapy management.
How long does groin injury rehabilitation take?
Rehabilitation typically progresses from the acute phase in the first week through functional conditioning at weeks 6–12, with return to play from week 12 onwards. The exact timeline depends on injury severity, tissue involved, and how consistently the athlete follows the progressive loading programme.
Does the Copenhagen Adduction Exercise prevent groin injuries?
The Copenhagen Adduction Exercise reduces groin injury risk when performed with adequate training volume and progressive overload. A 2026 systematic review confirmed its benefits for eccentric hip adduction strength and symptom reduction, but it works best as part of a multifaceted prevention programme rather than as a standalone intervention.
Recommended