
Multidisciplinary therapy terminology guide for professionals
- 1 day ago
- 8 min read

TL;DR:
Multidisciplinary therapy terminology creates a shared language for teams to coordinate patient care effectively. Mastering this language reduces communication errors, enhances collaboration, and improves patient engagement and outcomes.
Multidisciplinary therapy terminology is the shared clinical language that enables healthcare professionals from different disciplines to coordinate patient care without confusion or duplication. A multidisciplinary team (MDT) is defined as a collaborative group of professionals from diverse disciplines who coordinate care addressing physical, emotional, and social needs. Without this shared vocabulary, even well-staffed teams lose efficiency, and patients receive fragmented care. This guide covers the core terms, role definitions, therapy modalities, and the critical distinctions between multidisciplinary, interdisciplinary, and interprofessional care models. Mastering this language is not optional for clinical professionals. It directly shapes treatment outcomes.
What is the multidisciplinary therapy terminology guide covering?
A multidisciplinary therapy terminology guide organises the clinical vocabulary used across team-based care settings. The terms covered span team composition, therapy modalities, care coordination frameworks, and communication protocols. Professionals who work in physiotherapy, podiatry, acupuncture, mental health, and sports injury treatment all operate within these frameworks, whether they label them explicitly or not. Parkstherapycentre, established in 1986 across Bedfordshire and Buckinghamshire, applies exactly this kind of coordinated, team-based approach in daily clinical practice.
Core terminology and roles within multidisciplinary therapy teams
An MDT is not simply a group of specialists working in the same building. Regular meetings, shared decision-making, and integrated care plans are the structural components that make a team genuinely multidisciplinary. Without those structures, professionals work in parallel rather than together.

Who sits on a typical MDT?
A standard MDT includes psychiatrists, physiotherapists, nurses, social workers, occupational therapists, and dietitians. Each member contributes discipline-specific expertise while contributing to a shared patient goal. The team may also include speech and language therapists, podiatrists, and clinical psychologists depending on the patient’s presentation.
Common role responsibilities within an MDT include:
Physiotherapist: Assesses and treats movement disorders, pain, and physical rehabilitation needs.
Psychiatrist or psychologist: Manages mental health diagnoses, prescribes medication, and leads psychological interventions.
Nurse or specialist nurse: Coordinates day-to-day care, monitors progress, and liaises between team members.
Social worker: Addresses social determinants of health, housing, and community support.
Occupational therapist: Focuses on functional independence and daily living skills.
Podiatrist: Manages lower limb and foot conditions, particularly in complex or diabetic cases.
You may also encounter the terms cross-functional team and integrated care team used interchangeably with MDT in NHS documentation. These labels describe the same collaborative structure, though integrated care team often implies a broader community-based remit.
Team leadership in multidisciplinary models often defaults to the discipline with the highest perceived agency, which can marginalise allied health roles such as physiotherapy or podiatry. Recognising this dynamic is the first step to addressing it.
Pro Tip: When joining a new MDT, ask explicitly who chairs the meeting and who holds the final decision on the care plan. That answer tells you more about the team’s actual structure than any organisational chart.
What therapy modalities appear most in multidisciplinary settings?
Therapy modalities are the specific treatment methods a clinician uses within a care plan. CBT, DBT, and ACT are the three psychological modalities most frequently referenced in multidisciplinary treatment glossaries. Sessions typically last 60 minutes and occur weekly or bi-weekly. Manual therapy, physiotherapy techniques, acupuncture, and podiatric interventions complete the physical side of most multidisciplinary programmes.
Comparison of common therapy modalities
Modality | Full name | Primary aim | Typical use case |
CBT | Cognitive Behavioural Therapy | Restructure unhelpful thought patterns | Anxiety, depression, chronic pain |
DBT | Dialectical Behaviour Therapy | Regulate emotion and improve distress tolerance | Borderline personality disorder, self-harm |
ACT | Acceptance and Commitment Therapy | Build psychological flexibility | Chronic illness, trauma, burnout |
Manual therapy | Hands-on physical treatment | Restore joint and soft tissue function | Musculoskeletal pain, sports injuries |
Physiotherapy | Physical rehabilitation | Restore movement and function | Post-surgical recovery, neurological conditions |
Acupuncture | Needle-based treatment | Reduce pain and support recovery | Chronic pain, headaches, musculoskeletal issues |
Understanding the distinction between individual therapy and group therapy also matters in multidisciplinary clinic terminology. Individual sessions address patient-specific goals. Group sessions, common in mental health and pain management programmes, use shared experience and peer support as therapeutic tools. Outpatient programmes typically combine both formats across a structured timetable.
For a practical overview of physical treatment approaches, the types of physiotherapy techniques guide from Parkstherapycentre covers current modalities in detail.
Pro Tip: When documenting a patient’s care plan, always name the modality and its goal explicitly. Writing “CBT to address catastrophising around pain” is far more useful to the wider team than “psychological support.”
Multidisciplinary vs interdisciplinary vs interprofessional: what is the difference?
These three terms are not synonyms. Conflating them causes real confusion in team meetings, referral letters, and care planning documents. The distinctions matter practically, not just academically.
Multidisciplinary and interprofessional teams differ in a fundamental way. Multidisciplinary teams often function in parallel, with limited cross-discipline interaction. Each professional assesses and treats within their own scope, then contributes findings to a shared record. Interprofessional teams use formal shared decision-making, with role flexibility and collective ownership of the care plan.
Comparison of care models
Term | Decision-making | Leadership | Interaction style |
Multidisciplinary | Discipline-specific, then shared | Hierarchical, led by senior clinician | Parallel, coordinated at meetings |
Interdisciplinary | Integrated, negotiated across roles | Shared, with designated lead | Active collaboration across disciplines |
Interprofessional | Fully shared, role-flexible | Flat hierarchy, collective authority | Continuous, blurred role boundaries |
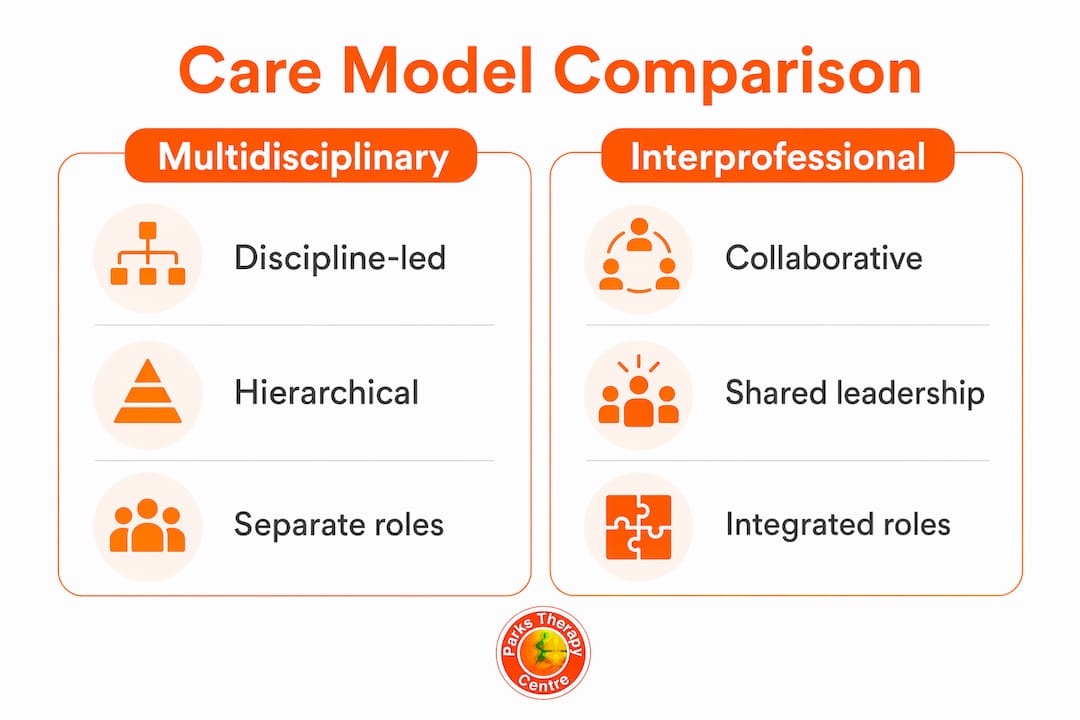
Multidisciplinary care focuses on patient outcomes with discipline-specific roles and hierarchical leadership. Interprofessional care emphasises team functioning and shared leadership. Interdisciplinary care sits between the two, with more integration than a traditional MDT but clearer role boundaries than a fully interprofessional model.
For professionals working in post-acute or care coordination settings, understanding these distinctions also shapes how referrals are written and how handover documentation is structured. A useful external reference for care coordination frameworks explains how these models translate into practical coordination levels.
Differentiating multidisciplinary from interprofessional terms is vital for setting appropriate communication expectations and improving team collaboration. A team that calls itself interprofessional but operates as a traditional MDT will consistently underdeliver on its stated goals.
How does terminology improve patient communication and outcomes?
Clear terminology reduces the information gaps that cause patients to disengage from their care. Normalising therapy terminology empowers patients to understand their care and communicate more effectively with their clinical team. Terminology familiarity also supports goal setting and improves therapy adherence.
Multidisciplinary clinics reduce wait times and costs by coordinating multiple specialist consultations into one structured visit. Many services are covered by insurance or state health programmes, which reduces the financial burden on patients. That efficiency only works when the team shares a common clinical language.
Patients in multidisciplinary models avoid fragmented appointments by receiving consolidated, team-based care. Direct specialist communication reduces informational gaps and improves clarity for both the patient and the team. This is particularly significant in complex cases involving chronic pain, neurological conditions, or multi-system presentations.
Practical steps for applying therapy language in clinical settings:
Use the modality name and its goal when writing referrals. Vague language produces vague responses.
Brief patients on key terms before their first MDT appointment. Patients who understand what an MDT is arrive better prepared.
Standardise terminology in shared records. Inconsistent labelling across disciplines creates confusion during handovers.
Review care plan language with the patient at each session. This keeps goals visible and reinforces shared ownership.
Educating both professionals and patients in therapy terminology increases patient engagement and therapy adherence. That is not a soft benefit. It translates directly into fewer missed appointments and more consistent treatment progress.
For complex pain presentations, the pain management strategies guide from Parkstherapycentre illustrates how CBT, ACT, and physical modalities are combined in practice.
Pro Tip: Create a one-page terminology sheet for patients entering a multidisciplinary programme. Include the names of their team members, their roles, and the modalities they will use. Patients who understand the structure engage with it far more consistently.
Key takeaways
Mastering multidisciplinary therapy terminology is the single most effective way to reduce communication failures, improve team cohesion, and increase patient engagement across integrated care settings.
Point | Details |
MDT structure requires formal processes | Regular meetings, shared decision-making, and integrated care plans define a genuine MDT. |
Modality names carry clinical meaning | Always name the therapy and its goal in documentation, not just the discipline. |
Multidisciplinary and interprofessional are not synonyms | Interprofessional teams use shared leadership; multidisciplinary teams typically use hierarchical leadership. |
Terminology empowers patients | Patients who understand their care plan engage more consistently and adhere to treatment. |
Coordinated care reduces costs and wait times | Multidisciplinary clinics consolidate specialist input, cutting duplication and patient burden. |
Why terminology precision changed how I think about team care
Working across clinical teams over many years, the single most consistent source of avoidable error is not clinical skill. It is language. Two professionals using the same word to mean different things, or different words to mean the same thing, creates gaps that patients fall through.
The distinction between multidisciplinary and interprofessional is a good example. Teams that claim to be interprofessional but retain a rigid hierarchy do not realise the benefits of shared decision-making. They carry the administrative overhead of collaboration without the clinical payoff. Naming the model accurately forces the team to examine whether their actual practice matches their stated approach.
Therapy language also shapes the patient relationship in ways that are easy to underestimate. A patient who knows what CBT is, why it has been recommended, and what a session involves arrives differently than one who has simply been told they are being referred to psychology. The first patient is a participant. The second is a recipient. That difference shows up in outcomes.
Formal training on therapy terminology is not yet standard in most undergraduate healthcare programmes. That gap is worth closing. Professionals who learn this vocabulary on the job absorb it inconsistently. A structured approach, whether through a multidisciplinary therapy terminology guide, a clinic-level glossary, or a dedicated induction module, produces more consistent results. The examples of multidisciplinary therapy approaches from Parkstherapycentre offer a practical starting point for teams building that shared foundation.
— Ivan
Parkstherapycentre and multidisciplinary care in practice
Parkstherapycentre has delivered team-based therapy across Bedfordshire and Buckinghamshire since 1986. The centre brings together physiotherapists, podiatrists, acupuncturists, and sports injury specialists under one coordinated approach, applying the same MDT principles this article describes.

For professionals and patients who want to understand how these services work together, the multidisciplinary physiotherapy page explains the centre’s integrated model in plain terms. Parkstherapycentre accepts insurance cover and offers online booking across multiple locations, making coordinated care accessible without the administrative friction that often accompanies specialist referrals.
FAQ
What is a multidisciplinary team in therapy?
A multidisciplinary team (MDT) is a group of professionals from different disciplines who coordinate care for a shared patient. Core components include regular meetings, shared decision-making, and integrated care plans.
How does multidisciplinary therapy differ from interprofessional care?
Multidisciplinary teams typically operate with hierarchical leadership and discipline-specific roles. Interprofessional teams use shared leadership, role flexibility, and continuous cross-discipline collaboration.
What therapy modalities are most common in multidisciplinary settings?
CBT, DBT, and ACT are the most frequently used psychological modalities. Physical modalities include manual therapy, physiotherapy, acupuncture, and podiatric treatment, often combined within a single care plan.
Why does therapy terminology matter for patient outcomes?
Patients who understand their care plan engage more consistently and adhere to treatment. Normalising therapy terminology empowers patients to communicate effectively with their clinical team and participate in goal setting.
What is the difference between interdisciplinary and multidisciplinary care?
Interdisciplinary care involves active collaboration and negotiated decision-making across roles. Multidisciplinary care coordinates discipline-specific contributions at shared meetings, with less continuous cross-role interaction.
Recommended