
Sports therapy terminology guide for injury recovery
- Mar 26
- 9 min read

You step into your physiotherapist’s office after a hamstring injury, and suddenly you’re bombarded with terms like AROM, PROM, eccentric loading, and the MEAT protocol. It feels like learning a foreign language when all you want is to get back to training. Understanding sports therapy terminology isn’t just about keeping up with your therapist’s explanations, it’s about taking an active role in your recovery, making informed decisions about treatment options, and communicating effectively with your healthcare team. This guide breaks down the essential terminology athletes and fitness professionals encounter during injury management and rehabilitation, transforming confusion into confidence.
Table of Contents
Key Takeaways
Point | Details |
Clear terminology | A clear grasp of terms such as AROM and PROM helps you participate actively in rehabilitation and make informed treatment decisions. |
Injury classifications | Knowing how strains and sprains are graded aids expectation setting and recovery timelines. |
MEAT protocol concept | Understanding Movement, Exercise, Analgesics and Treatment promotes controlled movement and early rehabilitation. |
Manual therapy roles | Joint mobilisation and IASTM have distinct roles, from reducing stiffness to breaking down adhesions. |
Recovery journaling | Keeping a recovery journal of ROM, pain and milestones helps track progress and inform adjustments. |
Essential sports therapy terms every athlete should know
When you start rehabilitation, your therapist will assess your Active Range of Motion (AROM), which measures how far you can move a joint using your own muscle power without assistance. This differs from Passive Range of Motion (PROM), where your therapist moves the joint for you while your muscles remain relaxed. The gap between these two measurements reveals important information about muscle strength, pain levels, and healing progress.
Understanding injury classifications helps you grasp the severity of your condition and expected recovery timeline. A strain affects muscles or tendons, whilst a sprain involves ligaments. Both injuries use a three-grade system: Grade 1 involves mild stretching with minimal tissue damage, Grade 2 includes partial tearing with moderate loss of function, and Grade 3 represents complete rupture requiring potentially longer rehabilitation or surgical intervention. Your therapist might describe a Grade 2 hamstring strain, immediately telling you to expect several weeks of structured rehab before returning to full training.
Common abbreviations you’ll encounter include:
ROM (Range of Motion): the measurement of movement around a specific joint
PT (Physical Therapy or Physiotherapy): the treatment profession focused on restoring movement and function
ATC (Athletic Trainer Certified): a healthcare professional specialising in injury prevention and emergency care
DTF (Deep Transverse Friction): a massage technique targeting scar tissue and adhesions
The MEAT Protocol represents modern thinking in acute injury management, standing for Movement, Exercise, Analgesics, and Treatment. This approach encourages controlled movement and early exercise rather than prolonged rest, accelerating tissue healing and maintaining fitness levels during recovery. Body mechanics refers to how you position and move your body during daily activities and sport, with proper mechanics reducing injury risk and supporting efficient movement patterns.
Pro Tip: Keep a recovery journal documenting ROM measurements, pain levels, and functional milestones. This creates a tangible record of progress and helps identify patterns that inform treatment adjustments.
Manual therapy techniques and their role in rehabilitation
Manual therapy encompasses hands-on techniques your physiotherapist uses to improve tissue mobility, reduce pain, and restore function. Joint mobilisation involves applying controlled, rhythmic movements to joints to increase ROM and decrease stiffness. Your therapist grades these mobilisations from 1 to 5, with lower grades addressing pain and higher grades targeting restricted movement. A Grade 3 mobilisation to your ankle after a sprain helps restore the gliding motion needed for normal walking and running mechanics.
Instrument-Assisted Soft Tissue Mobilisation (IASTM) uses specialised tools to detect and treat fascial restrictions, scar tissue, and chronic inflammation. The tools amplify what therapists feel in tissues, allowing precise treatment of problem areas. You might experience temporary redness or mild discomfort during treatment, but this technique effectively breaks down adhesions that limit movement and cause pain.

Muscle Energy Techniques (MET) require your active participation, using controlled muscle contractions against resistance provided by your therapist. This approach improves flexibility, corrects joint alignment, and reduces muscle tension through neurological mechanisms. During a hamstring MET treatment, you might push your heel against your therapist’s hand whilst they maintain resistance, followed by a gentle stretch that achieves greater lengthening than passive stretching alone.
Key manual therapy approaches include:
Strain-Counterstrain: identifying tender points and positioning your body to reduce pain and muscle spasm
Visceral Manipulation: addressing restrictions in organs and their connective tissues that may contribute to musculoskeletal pain
Myofascial Release: applying sustained pressure to fascial restrictions to restore tissue mobility
Trigger Point Therapy: deactivating hyperirritable spots in muscles that refer pain to other areas
Integrating manual therapy with exercise rehabilitation produces superior outcomes compared to either approach alone. Manual techniques prepare tissues for movement by reducing restrictions and pain, whilst exercises reinforce new movement patterns and build strength. This combination accelerates healing and reduces recurrence risk.
Pro Tip: Manual therapy effects typically last 48 to 72 hours, making this the optimal window for performing prescribed exercises that reinforce tissue changes and movement improvements.
Understanding prevention terminology and rehabilitation benchmarks
Prevention terminology in sports therapy creates significant confusion due to inconsistent definitions across clinical practice and research. Primary prevention traditionally aims to prevent injury occurrence in healthy populations through training modifications and screening programmes. Secondary prevention focuses on early detection and intervention when risk factors emerge, such as addressing muscle imbalances before they cause injury. Tertiary prevention manages existing injuries to prevent recurrence and minimise long-term consequences.
However, these definitions vary widely in sports medicine literature. Some sources classify immediate post-injury treatment as secondary prevention, whilst others reserve this term for risk factor management in uninjured athletes. This inconsistency complicates research comparisons and clinical guideline development. Standardised terminology would improve communication between practitioners, enhance research quality, and support evidence-based practice across sports therapy disciplines.
Rehabilitation benchmarks provide objective criteria for measuring recovery progress and guiding return-to-sport decisions. ACL reconstruction rehabilitation demonstrates the complexity of these benchmarks, with return-to-sport rates varying from 34% to 84% depending on study populations, surgical techniques, and rehabilitation protocols. This wide range highlights the importance of individualised assessment rather than relying solely on time-based protocols.
Injury type | Benchmark criteria | Typical timeline | Success rate |
ACL reconstruction | 90% limb symmetry in strength testing, hop tests, psychological readiness | 9-12 months | 34-84% return to pre-injury level |
Hamstring strain | MRI-confirmed tissue healing, isokinetic strength symmetry >90% | 3-12 weeks depending on grade | Variable based on severity |
Ankle sprain | Full pain-free ROM, single-leg balance >30 seconds, sport-specific testing | 2-8 weeks | 70-80% full recovery |
Shoulder instability | Rotator cuff strength symmetry, functional movement screening | 3-6 months | 60-90% depending on intervention |
Functional testing provides more reliable return-to-play indicators than time alone. Strength testing should demonstrate at least 90% symmetry between injured and uninjured limbs across multiple muscle groups. Hop tests assess power, landing mechanics, and confidence in the injured limb. Psychological readiness questionnaires identify fear of re-injury that may compromise performance or increase risk of subsequent problems.
Pro Tip: Track multiple benchmarks throughout rehabilitation rather than focusing on a single metric. Comprehensive assessment across strength, power, endurance, and psychological factors provides a complete picture of readiness to resume sport safely.
Comparing injury management protocols: MEAT versus RICE
The traditional RICE protocol (Rest, Ice, Compression, Elevation) dominated acute injury management for decades, emphasising immobilisation and passive treatments. However, modern evidence favours the MEAT protocol, which prioritises early movement and active rehabilitation. This shift reflects improved understanding of tissue healing and the detrimental effects of prolonged rest on muscle strength, joint mobility, and overall fitness.
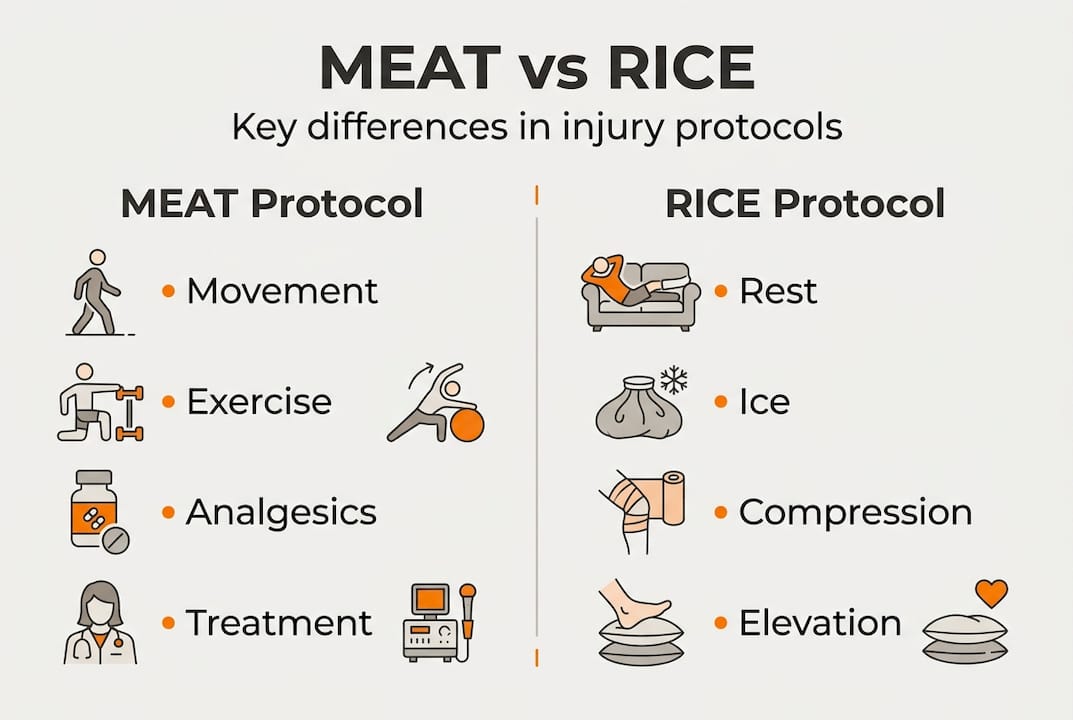
Protocol aspect | RICE approach | MEAT approach |
Primary focus | Rest and protection | Movement and exercise |
Activity level | Prolonged immobilisation | Early controlled movement |
Healing philosophy | Passive tissue recovery | Active tissue remodelling |
Strength maintenance | Often compromised | Prioritised throughout |
Return timeline | Potentially longer | Typically faster |
The MEAT protocol components work synergistically to optimise recovery. Movement maintains joint nutrition, prevents stiffness, and promotes proper collagen alignment during tissue healing. Exercise preserves strength and cardiovascular fitness whilst providing mechanical stimulus for tissue adaptation. Analgesics manage pain appropriately without masking important warning signals. Treatment encompasses various therapeutic interventions tailored to injury type and healing stage.
Applying the MEAT protocol to a Grade 2 ankle sprain follows this progression:
Begin gentle ankle circles and alphabet drawing within pain tolerance during the first 48 hours
Progress to partial weight-bearing walking with support as pain allows, typically days 2-4
Introduce resistance band exercises for ankle strengthening and stability once acute pain subsides
Add balance training on unstable surfaces to restore proprioception and prevent recurrence
Incorporate sport-specific movements and agility drills before full return to activity
Complete functional testing to confirm readiness for unrestricted participation
On-field rehabilitation (OFR) extends these principles to sport-specific contexts. The initial stage focuses on pain management and protecting healing tissues whilst maintaining general fitness through modified training. The intermediate stage reintroduces sport movements with reduced intensity and complexity, gradually increasing load as tissues adapt. The advanced stage involves full training participation with ongoing monitoring and adjustment based on response.
Eccentric training plays a crucial role in tendinopathy rehabilitation and injury prevention. This involves lengthening muscles under load, such as slowly lowering your heel below a step edge for Achilles tendinopathy. Eccentric exercises stimulate tendon remodelling, increase strength, and improve tissue capacity to handle sport demands. Research demonstrates superior outcomes compared to traditional rehabilitation approaches for many chronic tendon conditions.
The shift from RICE to MEAT reflects broader changes in rehabilitation philosophy. Rather than viewing injured tissues as fragile structures requiring protection, modern approaches recognise that controlled mechanical loading promotes optimal healing and functional restoration. This doesn’t mean ignoring pain or pushing through significant discomfort, but rather finding the sweet spot where movement supports recovery without causing additional damage.
Enhance your recovery with expert support at Parks Therapy Centre
Navigating sports therapy terminology becomes significantly easier when working with experienced professionals who explain concepts clearly and tailor treatment to your specific needs. Understanding the language of rehabilitation empowers you to participate actively in recovery decisions and communicate effectively about your progress and concerns.

At Parks Therapy Centre, our multidisciplinary team combines expertise in physiotherapy, sports injury treatment, and rehabilitation to support your journey from injury to full function. We offer comprehensive diagnostic imaging referrals when detailed assessment is needed, ensuring accurate diagnosis that informs effective treatment planning. Our therapists stay current with evolving protocols like MEAT and evidence-based manual therapy techniques discussed throughout this guide. Whether you’re managing an acute injury or addressing chronic problems, we provide personalised care that respects your goals whilst prioritising safe, effective recovery.
FAQ
What is the difference between a strain and a sprain?
A strain injures muscles or tendons (tissues connecting muscles to bones), whilst a sprain affects ligaments (tissues connecting bones to other bones). Both use a three-grade classification system based on severity. Strains typically result from overstretching or overloading during muscle contraction, causing pain and weakness. Sprains occur when joints move beyond normal ROM, creating instability and swelling around the affected area.
Why is the MEAT protocol preferred over RICE in modern sports injury management?
The MEAT protocol accelerates healing by promoting controlled movement and exercise that stimulate proper tissue remodelling and maintain fitness levels during recovery. Research shows prolonged rest from RICE approaches can lead to muscle atrophy, joint stiffness, and delayed return to activity. Early movement within pain tolerance improves outcomes for most soft tissue injuries. The MEAT approach also addresses psychological aspects of recovery by keeping athletes engaged in modified training rather than completely sidelined.
How can athletes use range of motion (ROM) measurements during recovery?
Tracking both active and passive ROM provides objective data about healing progress and identifies specific limitations requiring targeted treatment. Active ROM reveals muscle strength and control, whilst passive ROM shows joint and soft tissue restrictions. Comparing injured side measurements to your uninjured side establishes symmetry goals for rehabilitation. Regular ROM assessment helps you and your therapist adjust treatment intensity and progression timing based on measurable improvements rather than arbitrary timelines.
What are common manual therapy techniques and when are they used?
Joint mobilisation addresses stiffness and restricted movement after injuries or surgery, applying graded forces to restore normal joint mechanics. Instrument-Assisted Soft Tissue Mobilisation (IASTM) treats fascial restrictions and scar tissue limiting tissue mobility. Muscle Energy Techniques use your controlled contractions to improve flexibility and correct alignment issues. Each technique suits different injury types and healing stages, with your therapist selecting approaches based on assessment findings and treatment goals.
Why is consistent injury prevention terminology important in sports therapy?
Inconsistent definitions of primary, secondary, and tertiary prevention create confusion when comparing research studies and developing clinical guidelines across different healthcare settings. Standardised terminology improves communication between practitioners, supports evidence synthesis for treatment recommendations, and helps athletes understand prevention strategies at different injury risk stages. Clear language also facilitates better research design and outcome measurement in injury prevention studies. The sports medicine community continues working toward consensus definitions that enhance both clinical practice and scientific advancement.
Recommended